
ORTHODONTICS
AN ALTERNATIVE METHOD FOR ACCESSING IMPACTED CANINE USING A COMPUTER-AIDED DYNAMIC NAVIGATION TECHNOLOGY
DOI: https://doi.org/10.25241/stomaeduj.2023.10(1-4).art.4
Janina Golob Deeb1
DMD, MS
Professor
Email: jgolobdeeb@vcu.edu
Daniel Hall1
DMD, MSD
Email: daniel.j.hall47@gmail.com
George R Deeb2
DDS, MD
Email: gdeeb@vcu.edu
Caroline K. Carrico3
PhD
Associate Professor
Email: ckcarrico@vcu.edu
Aniket B. Jadhav4
BDS
MDentSc MHA Associte Professor
Email: abjadhav@vcu.edu
Eser Tüfekçi5
DDS, MS, PhD, MSHA
Professor
Email: etufekci@vcu.edu
1Department of Periodontology, School of Dentistry, Virginia Commonwealth University, Richmond, VA 23298-0056, USA
2Department of Oral Maxillofacial Surgery, School of Dentistry, Virginia Commonwealth University, Richmond, VA 23298-0056, USA
3Department of Dental Public Health and Policy, School of Dentistry, Virginia Commonwealth University, Richmond, VA 23298-0056, USA
4Department of Oral Diagnostic Sciences, School of Dentistry, Virginia Commonwealth University, Richmond, VA 23298-0056, USA
5Department of Orthodontics, School of Dentistry, Virginia Commonwealth University, Richmond, VA 23298-0056, USA
*Corresponding author: Professor Janina Golob Deeb, DMD, MS. Department of Periodontics, School of Dentistry, Virginia Commonwealth University, Richmond, VA 23298-0566, USA. Tel/Fax: (804)828-4869; e-mail: jgolobdeeb@vcu.edu.
Abstract
Objective
This in-vitro study aimed to compare dynamic navigation guidance (DNG) to the freehand method for exposure of palatally impacted canines.
Materials and Methods
Eighteen models with bilaterally palatally impacted canines were fabricated from resin. The models were scanned, and canine exposure was planned on CBCT by either traditional or DNG approach by randomizing the method and side. The time to plan, prepare, and drill was recorded. The Initial and final size of the osteotomy was measured. Time and osteotomy sizes were compared by jaw and method using two-way ANOVA.
Results
Thirty-six teeth were exposed evenly distributed between techniques. The total volume for initial and final osteotomy was assessed. The preparation time was significantly longer for the DNG, on average 10:07 (min:sec) compared to 3:19 for freehand (p<.0001).
The time to locate the tooth was significantly different on the left side, with DNG taking approximately two minutes longer than freehand (2:03; p=.0423) but did not differ significantly on the right side (16.78s longer for freehand; p=.9809). The time to finish the procedure did not vary significantly based on the method (p=0.8342) or side of the model (p=.3441). The total time was significantly longer for DNG (7:48; p<.0001). The initial osteotomy was marginally significantly smaller for DNG on the right side by an average of 7.25mm3 (p=.1520). The difference on the left side was insignificant (0.81, p=0.9933). The total volume removed did not differ significantly between the two methods (p=0.88851) or on the side (p=0.7582).
Conclusion
DNG can be used for canine exposure; however, the method requires longer preparation and operation time.
Keywords: Computer-Aided Navigation Technology; Impacted Tooth; Maxillary Osteotomy; Dental Digital Surgery; Tooth Movement Techniques;
1. INTRODUCTION
Adult maxillary canines erupt into the dental arch around the age of 11 to 12 [1]. A canine is possibly impacted if it remains unerupted despite its root being completely developed or the contralateral tooth being erupted for at least six months with complete root formation [2]. Second to mandibular third molars, maxillary canines are the most commonly displaced or impacted teeth [3]. One- third of canine impactions are located labially or in the alveolus, while two-thirds are located palatally [4]. Palatally displaced canines (PDCs) cannot erupt naturally. Depending on the population, less than 1-3% of patients present with canine impactions, [5] of which 8% occur bilaterally [6].
Canine impactions often go unidentified beyond the normal expected eruption timeline because they typically erupt later in the sequence of maxillary teeth. In addition, the deciduous canine may be mistaken for the permanent canine due to the close resemblance between these teeth. On the panoramic radiographs of patients in mixed dentition, 78% of the impacted canines were identified when their cusp tips overlapped or were located mesial to the long axis of the erupted lateral incisor root [2]. Once identified, management often involves surgical exposure of the tooth, along with orthodontic treatment.
The surgical approaches traditionally utilized to facilitate exposure of the impacted canines include open and closed techniques [9]. With developments in Cone-Beam Computed Tomography (CBCT) imagingtechnology, thelocationofimpactedcanines and their proximity to other teeth can now be easily determined. An accurate and better visualization of impacted canines in three dimensions is the key to the efficient and successful management of surgical exposure procedures [10].
Recently, a computer-aided system called dynamic navigation guidance (DNG) has been explored in implant dentistry and endodontics [11–13]. This technology enables the operator to pre-plan the osteotomy for optimal access to the impacted tooth with the aid of computer software on a preoperative CBCT. This virtual access is then turned into guided access with the help of computer software, fiducial landmarks, and a stereolithic camera that guides the drill directly to the desired location [14] Dynamic navigation guidance systems allow the surgeon to visualize the osteotomy and implant site entirely during preparation. The monitor provides real-time video feedback, which guides the osteotomy and minimizes positional deviations.
Applications of DNG have been explored and documented in endodontics and implantology, however no evidence exists at present on the feasibility of its application in orthodontics for uncovering impacted canine teeth. The primary objective for this study was therefore to explore the potential use of DNG approach in guiding access to palatally impacted canines. The second objective was to assess the time to plan and perform the canine exposure, the size of the initial access, and the final size of the osteotomy needed to completely uncover the impacted tooth achieved via DNG and compare it to a free-hand approach.
2. METHODS AND MATERIALS
Three 3D-printed plastic maxillary models (Navident, Claronav, Canada) representing various clinical scenarios (clinic scenarios 1, 2, and 3) of impacted teeth and edentulous space configurations were chosen. Six replicas of each model type were fabricated, and each model’s left and right sides were considered as access sites, resulting in 36 tests.
In this study, the epoxy models with lead powder were used for radiopacity. First, the crowns of de-identified extracted teeth were individually wrapped in molding clay that served as follicle space. This configuration was chosen to simulate impacted canines, which were then randomly embedded within the epoxy bilaterally on the right and left palatal aspect of the dental arch, roughly in the canine location (Fig. 1A).
A preoperative (first) cone beam computed tomographic (CBCT 1) scan (CareStream Kodak 8100 3-D Cone Beam, Carestream Dental, Atlanta, GA) was obtained for each model, and the image was loaded into the dynamic navigation software (Navident, Claronav, Canada), where virtual surgical access to the impacted tooth was planned. (Fig. 1B)
Once the models were prepared, they were mounted in manikins on the dental chair, and tags were attached to the jaw and handpiece (Fig. 2).
The attached tags and a camera above the operating field provided live video feedback to guide the osteotomy along the pre-planned pathway to the target location. During the procedure, the computer screen displayed the CBCT plan and real-time feedback on the drill or instrument tip deviation from the ideal planned position (Fig. 3).
The handpiece was recalibrated for each model by placing the bur tip on three random points on the model. A randomization schedule determined the order of model type used (clinic scenarios 1, 2, and 3), the side of the model (left or right), and the method of access (freehand or dynamic guided). All procedures were performed by a third-year graduate student in periodontics with previous experience in surgical tooth exposure and no previous experience using computer-aided Dynamic Navigation Technology.
Following the initial osteotomy, a second CBCT (CBCT 2) was captured to measure the area of the initial access (IA). (Fig. 1C,D) The DNG technique allows only the planning of straight-line access, and therefore it was used for the IA osteotomy only. All osteotomies for both groups were then further enlarged by freehand method for complete uncovery of the impacted tooth to enable attachment of the orthodontic chain. The final CBCT (CBCT 3) was taken to measure the size of the final access (FA) osteotomies. (Fig. 1E,F) Each initial access was performed to be ideal, minimally invasive with the minimum material removed for the operator to locate the tooth in order to eventually completely uncover the impacted canine.
The CBCT scans were taken using Carestream Cone Beam CT scanner (CS-8100D, Carestream Dental LLC, Atlanta, GA, USA.) at 60kVp and 2mA with the Voxel size of 150µm. All scans were analyzed with the ITK/SNAP DICOM viewer (http://www.itksnap. org/download/snap), an open source medical image computing platform for biomedical research. A manual segmentation tool was used to segment the osteotomy opening on the right and left side. The images were evaluated in the axial, coronal and sagittal planes. With a manual segmentation paintbrush tool, a standard brush size of 5 was used to mark the consistent thickness of the voxels of the osteotomy opening. For each access on each model, two end points of the walls of the osteotomy sites were connected by the paintbrush marking and were confirmed in the all three planes for accuracy. The interpolation tool was then used to fill any gaps between markings due to the non-orthogonal nature of the anatomy. The software then automatically calculated the volume in mm3 and provided the 3D rendering of the osteotomy opening in the form of a 3D-disc.
The time to plan and prepare for each procedure, including the time to access and fully expose the canine, was determined using a stopwatch (Apple iPhone X, Apple Inc. Cupertino CA, USA). The time required for procedures guided by dynamic navigation included virtual planning of the access for the osteotomy and calibration of the handpiece recognition pattern tags. The time to plan and prepare the site started at the opening of the CBCT image and stopped once the operator was ready to begin the procedure. Both exposure methods were timed from the initial opening of the CBCT file until the operator had familiarized himself with the surgical site and prepared the appropriate access approach. The timer was stopped following the initial access when a new CBCT (CBCT 2) was taken, but it was started again for the operator to completely uncover the impacted canine. The final uncovery was performed solely using the freehanded method. All the steps in this study were performed by one single operator.
Statistical Methods
Two-way ANOVA models were used to test for differences in time and volume based on the side of the jaw (left vs. right) and the method (freehand vs. DNG). An interaction term allowed for differences in the effect of the technique based on the side of the jaw. Post hoc pairwise comparisons were performed with Tukey’s adjustment to account for multiple comparisons. SAS EG v.8.2 (SAS Institute, Cary, NC) was used for all analyses. The significance level was set at 0.05.
3. RESULTS
The time to prepare for the procedure was significantly longer for the DNG technique than for the freehand method (p<.0001). The preparation time was, on average, 10:07s for the DNG method and 3:19s for the freehand approach. The time to locate the tooth was significantly different on the left side of the models with the DNG, taking approximately 2 minutes longer than the freehand approach (2:03; p=.0423) but did not differ significantly on the right (16.78s longer for the freehand approach; p=.9809). The time to finish the procedure did not vary significantly based on the method (p=0.8342) or the side of the model (p=.3441). The total time was significantly longer for the DNG technique (7:48; p<.0001). (Fig. 4)
Based on a volumetric assessment, the size of the initial osteotomy was significantly smaller for DNG on the right side of the models by an average of 7.13mm3 (adjusted p=.0097). The difference on the models’ left side was not statisticaliy significant (1.86mm3, p=.9933).
Figure 5 displays the average entry volume by method and side of the jaw. The total volume removed did not differ significantly between the two methods (78.9 vs. 77.4mm3; p=.7793) or on the side of the model (79.1 vs. 77.2mm3, p=.7175). (Fig. 6)
4. DISCUSSION
This study aimed to investigate the application of dynamic navigation guidance for use in the surgical exposure of palatally impacted canines and compare it to the traditional freehand approach.
The use of DNG has been applied in various dental disciplines. A previous study reported that dynamically guided implant placement was more accurate than freehand implant placement in multiple planes of orientation, including angular deviation, platform positioning, and apical positioning [15]. Similarly, in endodontics, the DNG technique showed benefits such as conserving thr tooth structure and finding calcified canals with better accuracy [11,12,16]. Using DNG, the operator can access a pre-determined destination with remarkable accuracy within a small access field. Therefore, for surgical exposure of palatally impacted canines, DNG can provide minimally invasive access to the tooth with an overall smaller access osteotomy and less volume loss than the conventional freehand technique.
In this study, the volumetric analyses revealed that the average initial access sizes on both sides were smaller for the DNG technique, significantly on the right side (7.13mm3, adjusted p=.0097) and less on the left side (1.86mm3, p=.9933). This difference favored DNG as a more accurate, direct, and less invasive approach. The difference between the left and right sides can likely be attributed to direct visualization on the left- hand side for a right-handed operator versus the right side, which may be more difficult to visualize with the freehand approach but is unaffected by a computer-guided dynamically navigated procedure. Our findings support that DNG could be used for the sites with difficult visualization and demonstrates quantitatively the differences in access osteotomy size. (Fig. 4) To the best of the authors’ knowledge, this is the first application of this technology to uncover palatally impacted canines. As such, no other studies are available for direct comparison. In orthodontics, it is crucial to utilize a method that does not harm the surrounding area when accessing an impacted canine, especially if there is contact with the lateral and central incisor.
The extrapolation of relevant findings could be interpreted in several ways. First, with less than adequate visualization for a right-handed operator, the DNG allows more controlled, precise access in more difficult operator conditions. The assistance that the DNG provides is reflected in a significantly smaller initial osteotomy and significant differences in volume sizes. On the left side, the differences were less significant due to direct vision and better visualization of the surgical site. Similar side-specific differences have been reported with less accurate implant placement on maxillary left sites than on contralateral right sites [13]. The differences may be attributed to working across the arch, angulation, and more challenging accessibility while maintaining the orientation of the jaw and handpiece tags within the tracking field of view for the left side.
While the size of the initial osteotomy was significantly smaller for the DNG, the size of the final osteotomy and total volume removed did not differ significantly between the two methods or the side of the model as the enlargement of IA to FA was achieved by freehand technique for both groups. Since access with DNG is essentially in a straight line, once the initial access is completed, the operator must continue to expose the impacted tooth using the freehanded method to ensure all bone and follicular structure that may impede the canine’s traction is removed. After finalizing the uncovery with freehand drilling, although the initial size of the access was smaller for DNG, we found that the final size of the structure removed was similar between the two methods.
If the accuracy and precision of DNG is its strength, the additional time needed in preparation for its use is its weakness. The time to prepare for the procedure was significantly longer for the DNG experiments (p<.0001). The preparation time was, on average, 10:07s for DNG and 3:19s for the freehand approach. The time to locate the tooth was significantly different on the left side of the models, with DNG taking approximately 2 minutes longer than freehand but did not differ significantly on the right. This finding supports our volumetric data, suggesting that the left side is more difficult for a right-handed operator, taking more time and resulting in larger, less precise access. The time to prepare the final osteotomy was similar based on the method (p=0.8342) or the side of the model (p=.3441) since all osteotomies were enlarged using the freehand technique. The total time was significantly longer for the DNG approach (7:48s; p<.0001).
The dynamic navigation guidance method could be a valuable tool in impacted tooth uncovering in clinical situations with proximity to vital structures, adjacent roots, or deep impactions with rotated teeth. The advantages of DNG drilling include real-time visualization, minimal collateral morbidity, pre-determined access, accuracy, and conservation of tooth structure [12,15]. Accuracy and precision of the initial access to the location of the tooth appear to be the main benefit associated with this application of the DNG technology. The downside of its use is the additional time, equipment cost, learning curve to use the system, and difficult access in some areas due to tracking tags.
Previous studies evaluating the operator learning curve using this technology found only slight improvements in time and accuracy of implant placement between the second and third attempts.13 Computer-guided simulation is used in other surgical fields such as laparoscopy and endoscopy, for training and evaluation of the surgical capacity and has demonstrated a learning curve and improvement with more training [17–19].
There are limitations to this study. First, the jaw tag was fixed to the typodont rather than individual models. Second, no simulation of soft tissue for mucoperiosteal flap elevation was provided on models, which influenced the time necessary for each procedure. Elevation of a mucoperiosteal flap would have added time to the traditional freehand surgical approach. Using the DNG approach with precisely planned access to the tooth, a surgeon may feel confident in the pre-planned procedure and pass directly through the palatal tissues to uncover the tooth without raising a flap. With the traditional approach lacking this precise access to the tooth, the elevation of the flap is inevitable. Precise access without a flap would reduce the overall time of the DNG procedure and decrease post-operative morbidity. An orthodontic chain can be passed through a window or tunnel through ablated palatal tissues if the tooth position can be accurately and predictably accessed [20]. Conversely, if a flap is raised to locate and expose the impacted tooth, the procedure affects a much larger area, requires a larger area of local anesthesia, takes a long time to elevate the flap and suture it back, and leads to higher intraoperative bleeding and post-operative morbidity. The total time of the procedures studied here is within the reported ranges in the literature. Access to palatally impacted canines required 12:1 minutes for freehand and 19.92 minutes for dynamic navigation guidance. On average, the mean operating time previously reported for a closed eruption technique was three times longer (36 min) than the open method (12 min) [21]. A potential drawback to not reflecting a full-thickness mucoperiosteal flap and complete visualization of the palatal bone could be insufficient osseous removal. Crowns do not contain the cells necessary to resorb bone and the crowns may move very slowly or not at all, giving the appearance of ankylosis. The periodontal health of palatally impacted canines has been the subject of several studies [22–25]. Previous studies concluded that when a conservative surgical technique is used, and the periodontium is kept healthy, periodontal attachment loss does not occur during orthodontic tooth movement [26,27].
5. CONCLUSION
The advantages of the DNG approach to access impacted canines are real-time visualization, accuracy, minimal collateral morbidity, and pre-determined access in situations with proximity to vital structures. Appropriate clinical circumstances may support the use of DNG despite the more time-consuming and technology-advanced process that includes additional treatment time, equipment cost, and operator learning curve.
Notes
fn1Citation: Golob Deeb J, Hall D, Deeb GR, Carrico CK, Jadhav AB, Tüfekçi E. An alternative method for accessing impacted canine using a computer-aided dynamic navigation technology. Stoma Edu J. 2023;9(1-4):32-38.
AUTHOR CONTRIBUTIONS
JGD and GRD conceived the ideas. JGD and DH conceptualized the study design, investigation and methodology. JGD supervised the manuscript writing, authors DH and AJ performed radiographic assessment and analysis and contributed to the manuscript writing. DH collected and curated the data and images. CKC was responsible for data curation and analysis, methodology. ET was responsible for interpretation of data and results.
ACKNOWLEDGMENTS
The authors would like to thank Navident (Navident, ClaroNav, Toronto, ON, Canada) for the donated materials and their technical support to make this study possible.
DECLARATIONS OF INTEREST
Materials donated from Navident (Navident, ClaroNav, Toronto, ON, Canada) included jaw models and tags.
References
- Hägg U, Taranger J. Timing of tooth emergence. A prospective longitudinal study of Swedish urban children from birth to 18 years. Swed Dent J. 1986;10 5:195-206.
PubMed Google Scholar Scopus WoS
- Lindauer SJ, Rubenstein LK, Hang WM, et al. Canine impaction identified early with panoramic radiographs. J Am Dent Assoc 1939. 1992;123(3):91-92, 95-97.
Full text links CrossRef PubMed Google Scholar Scopus WoS
- Thilander B, Myrberg N. The prevalence of malocclusion in Swedish schoolchildren. Eur J Oral Sci. 1973;81(1):12-20.
Full text links CrossRef PubMed Google Scholar Scopus
- Kokich V. Surgical and orthodontic management of impacted maxillary canines. Am J Orthod Dentofac Orthop. 2004;
126:278-283.
Full text links CrossRef PubMed Google Scholar
- Bishara SE, Ortho. D. Impacted maxillary canines: A review. Am J Orthod Dentofacial Orthop. 1992;101(2):159-171.
Full text links PubMed Google Scholar
- Peck S, Peck L, Kataja M. The palatally displaced canine as a dental anomaly of genetic origin. Angle Orthod. 1994;64(4): 249-256.
Full text links PubMed Google Scholar Scopus WoS
- Jacoby H. The etiology of maxillary canine impactions. Am J Orthod. 1983;84(2):125-132.
Full text links CrossRef PubMed Google Scholar
- Becker A, Shpack N, Shteyer A. Attachment bonding to impacted teeth at the time of surgical exposure. Eur J Orthod. 1996;18(5):457-463.
Full text links CrossRef PubMed Google Scholar Scopus WoS
- Johnston WD. Treatment of palatally impacted canine teeth. Am J Orthod. 1969;56 6:589-596.
Google Scholar
- Kau CH, Božič M, English J, et al. Cone-beam computed tomography of the maxillofacial region-an update. Int J Med Robot. 2009;5(4):366-380.
Full text links CrossRef PubMed Google Scholar Scopus WoS
- Saunders M. Achieving Dentin Conservation using Dynamic Navigation Technology for Locating Calcified Canals. VCU Theses Diss. Published online 2020.
CrossRef Google Scholar
- Jain SD, Saunders MW, Carrico CK, et al. Dynamically navigated versus freehand access cavity preparation: a comparative study on substance loss using simulated calcified canals. J Endod. 2020;46(11):1745-1751.
Full text links CrossRef PubMed Google Scholar Scopus WoS
- Golob Deeb J, Bencharit S, Carrico C, et al. Exploring training dental implant placement using computer-guided implant navigation system for predoctoral students: A pilot study. Eur J Dent Educ. 2019;23.
Full text links CrossRef PubMed Google Scholar Scopus WoS
- Block MS, Emery RW. Static or dynamic navigation for implant placement-choosing the method of guidance. J Oral Maxillofac Surg. 2016;74(2):269-277.
Full text links CrossRef PubMed Google Scholar Scopus WoS
- Block MS, Emery RW, Cullum DR, Sheikh A. Implant placement is more accurate using dynamic navigation. J Oral Maxillofac Surg. 2017;75(7):1377-1386.
Full text links CrossRef PubMed Google Scholar WoS
- Zubizarreta-Macho Á, Muñoz A de P, Deglow ER, et al. Accuracy of computer-aided dynamic navigation compared to computer-aided static procedure for endodontic access cavities: an in vitro study. J Clin Med. 2020;9(1):129.
Full text links CrossRef PubMed Google Scholar Scopus WoS
- Schijven MP, Jakimowicz J. The learning curve on the Xitact LS 500 laparoscopy simulator: profiles of performance. Surg Endosc Interv Tech. 2004;18(1):121-127.
Full text links CrossRef PubMed Google Scholar Scopus WoS
- Aggarwal R, Black SA, Hance J, et al. Virtual reality simulation training can improve inexperienced surgeons’ endovascular skills. Eur J Vasc Endovasc Surg. 2006;31 6:588-593.
Full text links CrossRef PubMed Google Scholar Scopus WoS
- Verdaasdonk EGG, Stassen LPS, Schijven MP, Dankelman J. Construct validity and assessment of the learning curve for the SIMENDO endoscopic simulator. Surg Endosc. 2007;21(8): 1406-1412.
Full text links CrossRef PubMed Google Scholar Scopus WoS
- Crescini A, Clauser C, Giorgetti R, et al. Tunnel traction of infraosseous impacted maxillary canines. A three-year periodontal follow-up. Am J Orthod Dentofacial Orthop. 1994;105(1):61-72.
Full text links CrossRef PubMed Google Scholar Scopus
- Pearson MH, Robinson SN, Reed R, et al. Management of palatally impacted canines: the findings of a collaborative study. Eur J Orthod. 1997;19(5):511-515.
Full text links CrossRef PubMed Google Scholar Scopus WoS
- Wisth PJ, Norderval K, Boe OE. Periodontal status of orthodontically treated impacted maxillary canines. Angle Orthod. 1976;46(1):69-76.
Full text links PubMed Google Scholar Scopus
- Hansson C, Rindler A. Periodontal conditions following surgical and orthodontic treatment of palatally impacted maxillary canines-a follow-up study. Angle Orthod. 998;68(2):167-172.
Full text links PubMed Google Scholar Scopus WoS
- Becker A, Kohavi D, Zilberman Y. Periodontal status following the alignment of palatally impacted canine teeth. Am J Orthod. 1983;84 4:332-336.
CrossRef PubMed Google Scholar Scopus
- Boyd RL. Clinical assessment of injuries in orthodontic movement of impacted teeth. Am J Orthod. 1984;86(5):407-418.
CrossRef PubMed Google Scholar
- Ericsson I, Thilander B. Orthodontic forces and recurrence of periodontal disease: An experimental study in the dog. Am J Orthod. 1978;74(1):41-50.
CrossRef PubMed Google Scholar Scopus
- Caprioglio A, Vanni A, Bolamperti L. Long-term periodontal response to orthodontic treatment of palatally impacted maxillary canines. Eur J Orthod. 2013;35(3):323-328.
Full text links CrossRef PubMed Google Scholar Scopus WoS

Janina GOLOB DEEB
DMD, MS, Professor, Department of Periodontology, School of Dentistry Virginia Commonwealth University Richmond, VA, USA
CV
Dr. Janina Golob Deeb graduated from the University of Ljubljana, Slovenia (1996), degree from the University of Ljubljana, Slovenia, and from the Oregon Health Sciences University with a certificate in Periodontology (2000) and a Master in Science degree (2001). Dr. Golob Deeb is a board-certified periodontist and serves as Director of Predoctoral Periodontics in the Department of Periodontology at the Virginia Commonwealth University School of Dentistry. Her clinical and research experience in applications of Dynamic Navigation Technology have focused on dental implantology, endodontics, uncovering of impacted teeth, and its effectiveness as a tool in skill development in implant placement.
Questions
- Which of the following is true for canine impactions?
- The majority of impactions are mid-alveolar;
- The majority of impactions are labial;
- The majority of impactions are palatal;
- The location of impactions is equally distributed between the buccal and palatal aspects.
- Canine impactions often go unidentified beyond the normal expected eruption timeline because:
- They typically erupt earlier in the sequence of maxillary teeth;
- They typically erupt later in the sequence of maxillary teeth;
- Deciduous canine may be mistaken for the permanent canine due to close resemblance;
- b and c.
- Which of the following imaging techniques depict accurate spatial relationships of the occult pathology in the jaws?
- Intraoral periapical radiograph;
- Panoramic radiographs;
- Nuclear scan;
- Cone beam computed.
- Dynamic Navigation Guidance has been explored for use in dentistry for:
- Implant placement;
- Endodontic therapy;
- Exposure of impacted teeth;
- All of the above.
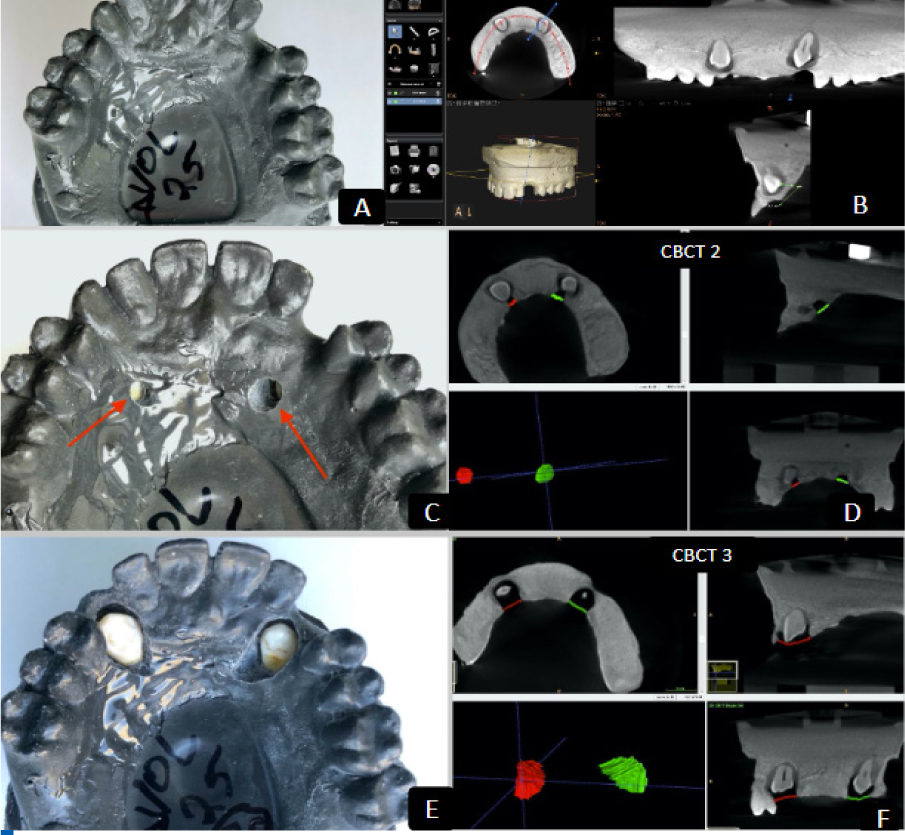
Figure 1A-F One of three maxillary models used in the study (A) with initial CBCT 1 of impacted canines (B). Preparation of Initial Access (IA) on the model (C), and volumetric analysis of IA on second CBCT 2 (D). Enlarged Final Access (FA) preparation for crown exposure (E), and volumetric analysis of FA on the third CBCT 3 (F).

Figure 2 Experimental set-up with typodont head and maxillary model on a dental chair (A), tracking tags attached to jaw (A) and handpiece (B) enable tracking during the navigated procedure.

Figure 3 Planned osteotomy access (yellow) with real-time positional feedback on virtual display (green).

Figure 4 Average procedure time by side and method (seconds).

Figure 5 Average entry volume by side and method.

Figure 6 Average total volume removed by side of the jaw and method.